 企業(yè)郵箱
企業(yè)郵箱






Clinical Study of Moist-Exposed Burns Ointment on Improving
作者:Rong Xiang Xu 出版社:KARGER 發(fā)行日期:In 2004 INTRODUCTION
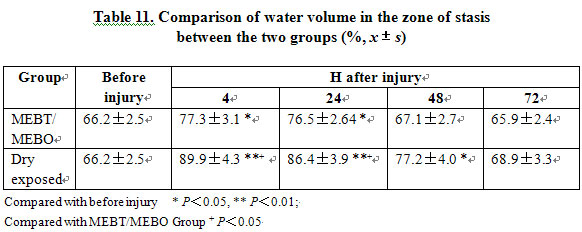
The typical changes in microcirculation immediately following burn trauma include cellular and gross anatomical changes. At the cellular level, we see an increase of vascular permeability and an increased risk of microthrombus. At the macro level, we see three concentric circles developing around the wound after cutaneous burns, ranging from interior to exterior and termed the zone of necrosis, the zone of stasis and the zone of hyperemia [1]. The microcirculation in the zone of stasis is characterized by the formation of progressive microthrombus. The location of the zone of stasis varies according to the depth of the burns. Burns affecting dermis are termed second-degree burns while third-degree burns involve the full-thickness of skin as well as subcutaneous tissues. The ultimate burn depth is determined by the development of the stasis zone, which may extend full-thickness, arresting blood circulation and causing tissue necrosis resulting in third-degree burn. However, if there is some improvement in the microcirculation in the zone of stasis, deep second-degree burns will rarely deteriorate into third-degree burns. BRT was designed to deal with the zone of stasis by improving the microcirculation, avoiding the formation of microthrombus and thereby arresting progressive necrosis.
Recent research suggests that significant release of vascular active factors in plasma, endothelin (ET) and nitric oxide (NO), has a close correlation with the deterioration of vulnerable tissue within the zone of stasis during the early postburn stage[2-4]. ET and NO released from the burn wound become the primary source of ET and NO in plasma. The studies during the previous decade have paid great attention to ET and NO known as “star molecules” because they are the most powerful vascular contraction and dilation factors known to man. Under normal non-traumatic situations, vascular endothelial cells maintain a relatively stable ratio of ET/NO to ensure the normal capacity for vasoconstriction and dilation within the microcirculation of the skin. However, certain pathological conditions such as stress, ischemia, hypoxia and acidosis may stimulate the massive increase in the synthesis and release of ET and NO. These challenges upset the original balance of ET and NO, causing a cascade of reactive pathological damages. This study investigates the relative impact on plasma ET/NO ratio by BRT (MEBT) and conventional therapies and gives a further investigation on the mechanism of MEBO for improving the microcirculation of burns wounds.
MATERIALS AND METHODS
The study involved 34 adult patients suffered 30~40% TBSA burns with more than 20% TBSA of deep second-degree wounds, all of whom were admitted to the hospital at 4~5 h after injury. All subjects were randomized to receive either BRT with MEBT/MEBO or conventional dry-expose therapy. The MEBO group included 18 patients (11 male, 7 female) with a mean age of 26±10.9 years while the dry-exposed group comprised 16 patients (10 male, 6 female) with a mean age of 28±12.0 years.
All patients were treated with the standard of care as regards fluid supplement, anti-infection and anti-inflammation. For the BRT with MEBT/MEBO group, MEBO ointment was spread at a thickness of 1 mm guided by the following principles: replace the ointment every 4~6 h during the exudation and repair periods; during the liquefaction period, the intervals of reapplying MEBO is determined by the amount of liquefied products on the wound. The typical interval calls for reapplication every 4 h. The patients receiving the dry-exposed therapy received topical debridement and were treated with 1% silver surfadiazine (SD-Ag) daily.
Venous blood were sampled, respectively, from burn patients in both groups at 8 h, 1, 2, 3, 5, 7, 14 days postburn, and also from 5 healthy control males and females. NO was determined by the Griess method. ET was measured with radioimmunoassay (RIA). Both ET and NO kits were purchased from East Asia Immunity Technology Institute, General Hospital of CPLA.
RESULTS
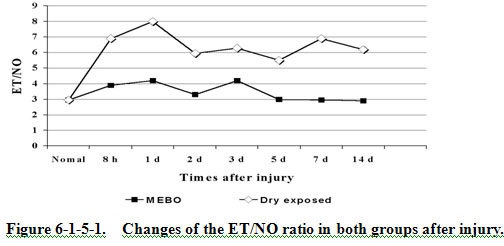
The normal level of ET in plasma was 42.812.2 pg/ml, NO: 14.53.6 mol/L, the ratio of ET/NO 2.95. Table 12 shows that ET in both groups markedly increased after injury, but we see that the increment in the BRT with MEBT/MEBO group was much lower than that in the dry-exposed group. The MEBO group returned to normal level on the 5th day postburn as compared to the dry-exposed group’s value remained at a high level even at day 14. Table 12 shows an obvious increase of NO in both groups at 8 h. In the BRT with MEBT/MEBO group, the NO gradually decreased to normal by day 3 compared to day 7 for the dry-exposed group. Figure 12 shows that the ratio of ET/NO in the BRT with MEBT/MEBO group decreased to 2.95 after 1 day, while that in the dry-exposed group remained much higher than 2.95 at all phases.
The MEBO group required 5.62.5 days to heal the superficial second-degree burns wounds and required 15.64.7 days for the resolution of deep second-degree wounds as evidenced by good skin elasticity and no scar formation. In the dry-exposed group, 8.74.6 days were required for healing superficial second-degree burns wounds, and 21.66.4 days were required for the completion of healing in deep second-degree wounds. However, note that the end result of this protocol, as contrasted with the MEBO protocol was suboptimal as it resulted in scar formation and poor elasticity.
CONCLUSION
We have demonstrated that BRT with MEBT/MEBO improves the microcirculation of burns wounds, shortens healing time, and promotes deep second-degree wounds to heal without scar formation by means which include the optimization of the ratio of ET/NO.
DISCUSSION
The formation of progressive microthrombus in the zone of stasis may deepen and extend the area of burns wounds, thereby directly worsening both the rate of wound healing and the clinical prognosis. Therefore, an important question must be weighed by the world’s burns therapists: How can one best alleviate tissue damage, promote wound healing and reduce the possibility of scar formation? Current research suggests that BRT (MEBT) offers the best answer to these questions.
This study was designed to investigate the effect of MEBO on plasma ET/NO so as to further discover the mechanisms of MEBT therapy. ET, separated from supernatant fluid of cultured pig aorta endothelial cell by Yanagisawa in 1988, is mainly synthesized in the vascular endothelial cell and is known to be the strongest vasoconstrictive peptide in addition to other biological actions. However, the excessive release of ET may cause micro blood vessels to contract and spasm for an extended period of time, resulting in microthrombus formation. NO is a potent gaseous free radical and is synthesized in the cytoplasm of vascular endothelial cells, vascular smooth muscle cells, macrophages, platelet, etc. This reaction occurs when nitrogen monoxide synthetase (NOS) catalyzes the guanidin-end nitrogen of L-Arg to combine with oxygen. There are two types of NOS: constitutional NOS (cNOS) and inducible NOS (iNOS). NO has a very short half-life as it may react with circulating oxyhemoglobin, deoxyhemoglobin, superoxide anion or free oxygen to create stable products such as nitrite and nitrate. These are metabolized mainly through the kidney.
NO expresses its effects in two ways. On the one hand, NO is antagonistic with ET in dilating micro blood vessels, forming a protective layer in tunica intima, preventing platelet and neutrophil from adhering to the vessel wall and inhibiting the formation of microthrombus. On the other hand, the excessive release of NO may result in severe wound exudation and edema in the early stages postburn, thus increasing damage to tissues and cells. Under the normal situation, NO and ET maintain a certain dynamic equilbrium as an increase of ET promotes an elevation of NO synthesis while NO inhibits the synthesis of ET. A physiologic ratio of ET/NO represents a healthy balance.
According to the studies in recent years, the iNOS and ET mRNA genes located in burns wounds, heart, lung, kidney, liver and gastrointestinal tract express an increasing activity postburn, which leads to a massive release of ET and NO, especially from the wound. The significant increase of ET and NO in the circulation and the imbalance of ET/NO ratio have a close correlation with shock, acute renal failure, acute respiratory failure, stress ulcer and cerebral edema after severe burns. Great care must be paid to the role of ET/NO if one is to prevent progressive damage of the wound tissues in the zone of stasis at the early stages postburn [2]:
1. NO and ET, known as the most potent vasoconstriction and vasodilatory factors, should maintain a healthy balance during the critical postburn period.
2. The increment of NO and ET in blood plasma postburn has a positive relationship with the increase of the capillary permeability, leading to massive exudation and hyperedema [3, 4].
3. The increase of ET in plasma, the contraction and spasm of the micro blood vessels, the thrombus formation around the wound and underlying tissues, and edema pressure may cause secondary ischemia and necrosis to the adjacent tissues.
4. The exudates, being rich in protein, provide a good culture medium for bacteria growth.
It was found that the application of a non-selective ET receptor antagonist, AK-044, may alleviate the secondary damage to burns wounds resulting from the increase of ET [5]. In this study, the increment of ET and NO in the BRT with MEBT/MEBO group was obviously lower than that in the dry-exposed group. In the former group, the ET/NO ratio in plasma decreased after 1 day toward a normal level of 2.95, representing a timely improvement in the tissue microcirculation status particularly in the zone of stasis. This prevented the occurrence of progressive microthrombosis and prevented the progressive necrosis of tissue by optimizing the wound environment. In the dry-exposed group, ET and NO increased significantly at all phases and the ET/NO ratio in plasma remained much higher than normal level (2.95), usually at around 6. ET might play a dominant role in this change by keeping the micro blood vessel contracted and spasming for a long time resulting in microthrombosis, low vitality of wound tissues and poorer healing process compared to that in the BRT with MEBT/MEBO group. The results suggest that the BRT with MEBT/MEBO group is superior to the dry-exposed group in wound healing time and outcome. However, further study is yet to be conducted for the specific mechanism on how MEBO controls the adequate release of ET and NO from the burns wounds, and on how to promote the return of the ET/NO ratio to normal as rapidly as possible.
Reference
1. Bonaldi LA, Frank DH: Pathophysiology of the burn wound; In Achauer BM(ed): Management of the Burned Patient. Norwalk, Appleton & Lange, 1987, pp 21-47.
2. Battal MN, Hata Y, Matsuka K, et al: Reduction of progressive burn injury by using a new nonselective endothelin-A and endothelin-B receptor antagonist, Tak-044: an experimental study in rats. Plast Reconstr Surg 1997; 99: 1610-1619.
3. Kowal VA, Walenga JM, Sharp PM, et al: Postburn edema and related changes in interleukin-2, leukocytes, platelet activation, endothelin-1, and C1 esterase inhibitor. J Burn Care Rehabil 1997; 18: 99-103.
4. Sozumi T: The role of nitric oxide in vascular permeability after a thermal injury. Ann Plast Surg, 1997; 39: 272-277.
5. Jia XM, Zhu ZM, Zeng Q, et al: The dynamic changes of endothelin-1 in rat plasma, wound and organs at the early stages postburn. Med J PLA 1997, 22: 40-42.